If only Senator Proxmire and his Golden Fleece Award were still around! Perhaps he would call this the Golden Loofa -- A disappointing, shady version of "you scratch my back, I'll scratch yours."
The Background
Well over a decade ago, those involved in the fight against ALS have wanted a good, central census of people with ALS -- a complete, statistically meaningful nose count of the who, where, when of the incidence and prevalence of ALS.
The ALS Association proposed that the CDC create such a central "registry." That seemed like a good idea since individual state and private registries were counterproductive to getting a good national census.
ALSA (The ALS Association) has an annual advocacy legislative agenda. Funding was to be requested for "building block" projects. Seeds were sewn to have an ALS Registry enacted into law. The ALSA approach is for advocates not to worry about the technical details -- just tell your stories. We had little information about the project design or anticipated budget details. Many of us worked hard at our own expense to get the Registry passed. Certainly it was important for us to collect the dots if we ever were to connect the dots. The ALS Registry Act was finally signed into law in 2008.
https://www.govtrack.us/congress/bills/110/s1382
The annual dollars that we were to request to actually develop and deliver the Registry increased. Development of the Registry would be expensive. We received no businesslike itemization of the dollars we requested annually. ALSA told us what to ask for. We told our stories. We worked hard.
http://web.alsa.org/site/PageServer?pagename=ALS_Registry_Background#Congress
The project was "generously funded" (the words of the CDC project leader in 2010).
The design of the new Registry turned out to be based on passive data mining of government files -- Medicare, Medicaid, VA. People with ALS are eligible to get into those systems fairly quickly, so that looked like fertile ground for finding them (and avoiding any attempt at mandatory reporting of ALS as is done for cancers). The concept of a web portal for voluntary reporting was added to the base design. And we waited. The most recent government files are already several years old by the time the CDC could get them. Even though the web portal finally launched late in 2010, we couldn't get any data out until the passively-mined government files caught up. We were curious and asked about progress and patient uptake. In addition to the time lag excuse, ALSA staff told us that no information based on portal data entry could be released because of OMB rules. The OMB excuse came up repeatedly from ALSA as those of us anxious to know how things were going asked questions. The portal was clunky by 2010 standards. We wondered how many people with ALS were finding it and entering their data. Were there barriers that needed to be addressed? Our questions weren't answered.
Just tell your stories and continue to ask for unsubstantiated millions of dollars annually. We were good soldiers. We trusted. We believed. We didn't ask enough questions (not that they would have been answered anyway).
We weren't to get any until 2014. Keep being good advocates and ask for the annual appropriations you're told to request.
The Accidental Discovery
In June, 2013, I ran across something at usaspending.gov quite by accident. There were some large contracts handed (no-bid as the sole source for the services) to The ALS Association for "education and outreach" for the Registry. Surely this wasn't what it appeared to be! It was. The organization that works with the CDC and tells us the appropriation needed annually was actually a large contractor on this very project. And we had never been told.
https://docs.google.com/file/d/0B0yxxVCJLk5lOElWR2g0S2VvVzg/edit
The Concern
We were dumbfounded that ALSA was being paid to do what we thought our donations were already paying them to do -- to raise awareness of the Registry and to promote patient self-enrollment. And substantial taxpayer funds were being directed to ALSA without transparency or any competitive bidding. They failed to tell us! That's a pretty important tidbit since they are the ones who tell us advocates the grand sum to request (without any businesslike accounting of details) on Capitol Hill every year.
Add the fact that ALSA and MDA are the only ones allowed to nominate patient participants for the Registry annual meeting. It looked bad. It smelled bad. It was way too cozy for good oversight.
With a little more digging, we found that the MDA was about to be handed a no-bid contract of its own.
https://govtribe.com/project/als-outreach-and-education-activities-to-support-the-national-als-registry-2 Two sole sources? What was going on here? The phrase "
turn at the trough" came to mind.
The FOIA Request
I asked the CDC ATSDR ALS Registry administrator what work product, deliverables, and work standards were on those no-bid contracts. What were ALSA and MDA actually doing for those large sums? The response was that I would have to file a Freedom of Information Act request. What was a simple question took us on a long journey.

The FOIA requests I submitted in 2013 were simply for the work product, deliverables, and work standards for two of the contracts -- one for ALSA and one for the MDA.
And we waited.
The Wait
Fortunately I'm persistent and healthy (knock on wood). For over two years I followed up on the status of the requests. The CDC FOIA office form response was that these things can take years. Two of my friends with ALS who helped with the FOIA request died during the wait.
During the course of the wait, the first report from the ALS Registry was finally published in 2014, and it was certainly disappointing in substance. It raised a lot of questions about the completeness of the Registry. It raised a lot of concerns about self-enrollment. It yielded numbers that the very organizations that got big contracts on the projects don't seem to want to use, yet they continue to pat themselves on the back.
Any oversight on this project seems to be done by people with substantial financial interests in calling the project a success. Just tell your stories, advocates. There are always new, naive ALS advocates to take the places of those who start to ask questions like my buddies who died waiting for the FOIA requests. The annual meeting patient representatives are hand-picked by the contractors ALSA and MDA. And we've never seen the budget discussed in the minutes of those annual meetings.
And we continued to wait.
Finally, Two Contracts
In November 2015, after another status inquiry, a large envelope appeared in my mailbox. It contained a letter explaining some of information withheld along with a CD with two files. A CD. Who still has a computer with a CD drive? Oh, well, I'm persistent. Here they are: an
ALSA contract and an
MDA contract. Both have information redacted, but there's plenty there to substantiate concerns about these sweet deals.
ALSA's Deal
.
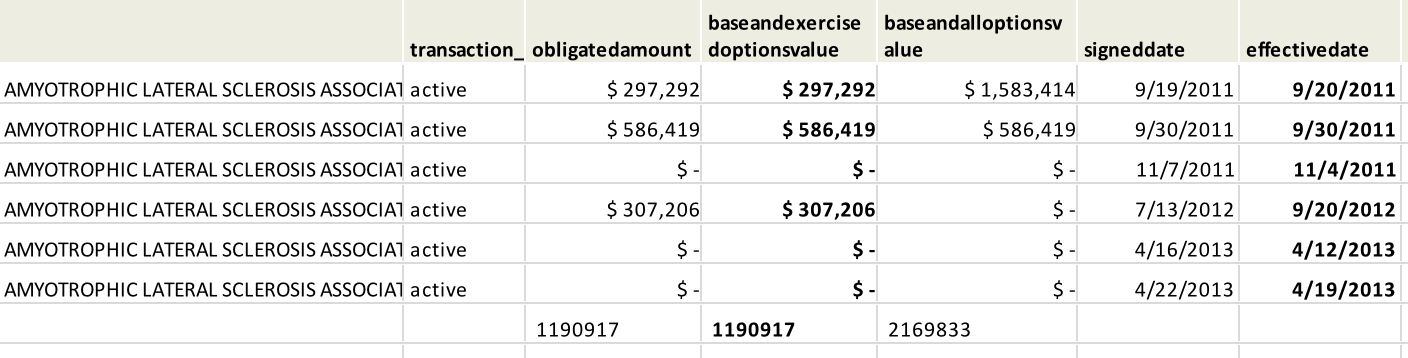
The first contract was signed on September 19, 2011 Keep in mind that the Registry had been promoted by ALSA for years before that and that the online portal for people to self-enroll had been opened in 2010.
The contract purpose is pretty a pretty vague "to promote the National ALS Registry through an exptensive nationawide network of ALS Clinics, Chapters, and Certified Centers of Excellence."
The "technical requirements" provide us with some deliverables that are things and tasks (and not Registry results). ALSA will fulfill their responsibilities by doing the things many of us thought they should do as part of their mission that we already support with donations. They are being paid to do tasks but there is no linkage to any results in increasing or even maintaining self-enrollment in the Registry. It's a pretty sweet deal, especially when you don't have to bid. And it amounted at that time to over $1.5 million over five years. But wait, there's more!
Less than two weeks after both parties signed the original contract, it was modified to an even bigger, sweeter deal. The amount was increased to a redacted amount. ALSA got the leeway to expand Registry education and outreach work to MLB, the NFL, MLS. And that has increased self-enrollment how? Again, there was still no tie or performance expectation to maintain or increase self-enrollment in the Registry.
And the seeds of scope creep were planted.
And in this bigger, better version of the contract, the monthly compliance-reporting requirement in the first contract was suddenly changed to, "To be discussed at Kick-off Meeting." OK, who was at that rather important Kick-off Meeting?
In both editions of the contract, there is a clear obligation that a contractor may not lobby for funding:
And we who go to the ALSA Advocacy Conference or who are online advocates hear about how great the Registry is from ALSA. ALSA employees tell us to ask our legislators for another $10 million. I suspect that through an intricate tapdance of who is on whose meter while talking to advocates, ALSA managed to fulfill the letter of that clause while defying its spirit.
There is also a requirement: "4. Educate and train Contractor's local chapters' staff to identify ALS patients, increase awareness about the National ALS Registry, and if necessary, provide assistance in registry enrollment. Contractor's chapter staff will not recruit ALS patients for the registry and will only assist with registration for those patients who request such assistance." Read that paragraph a few times and scratch your head.
There are pages and pages in that pdf that was on the CD, and it's not easy reading for a lot of reasons. By the time you plow to the end, you see a contract that somehow grew to $2.2 million.
A copy of some pages of the contract with my comments
is here. I will call them lowlights rather than highlights.
MDA's Deal
The MDA no-bid contract was dated September 12, 2013, two years after ALSA had received its no-bid contract. The amount is a whopping $2,695,642 over five years. It has another interesting clause: "The contractor chosen must have direct and proprietary access to a high percentage of ALS patients in the United States." Chosen? Proprietary access?
In the base year MDA was to produce a Registry toolkit whose requirements are remarkably like we just paid ALSA to do. Why not just use ALSA's, folks?
MDA got the same missive as ALSA to supply "relevant equipment" to district offices, clinics, and support groups help promote the registry. There is no standard for "relevant equipment" nor is there any accountability. That's kind of hard to swallow when we see how hard people with ALS have had to fight government rules to supply them basic communication technology.
MDA is also being paid to educate its own "stakeholders" about the differences between the CDC's ALS Registry and other ALS-related registries. You see, MDA launched its own registry after the CDC's launched. Now we pay the launcher to clear that up among its own "stakeholders." Perhaps they can enlighten us on comparative data at the annual CDC Registry meeting sometime.
And maybe at the next CDC Registry meeting each invitee will introduce herself or himself as a project contractor, if appropriate. And perhaps the patient and caregiver representatives will tell us which ALS organization nominated them for participation.
Our Deal
We got the dirty deal. We got a national Registry with significant design flaws. We got poor execution. We got insider oversight and no accountability. We got a project whose scope was allowed to creep to fit a very generous, unsubstantiated budget. We got a project that continues to grow in search of things it might do well. We got a cozy, secretive relationship that defies the spirit of government rules that prohibit agencies and contractors lobbying for funds. We got a dirty deal. People with ALS were fleeced. We taxpayer-advocates were fleeced. Or loofaed.