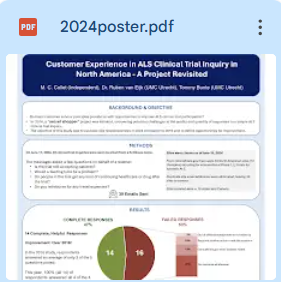
In 2016, the secret shopper project showed some customer service gaps that could be holding back clinical trial enrollment in ALS.
Are things better in 2024?
The poster tells the story --

In 2016, the secret shopper project showed some customer service gaps that could be holding back clinical trial enrollment in ALS.
Are things better in 2024?
The poster tells the story --
The CDC ALS Registry is a product of the Agency for Toxic Substances and Disease Registry (ATSDR), a government agency, generously funded by American taxpayers.
In the ALS Registry Act of 2008, ATSDR was given the primary mission of the ALS Registry -- "better describing the incidence and prevalence of ALS in the United States." That's the mission that should be hanging over every desk and computer of those paid to work on this project. It should guide every work product.
But it doesn't.
We have a new report publication from the Registry staff -- "Prevalence of ALS in all 50 states in the United States, data from the National ALS Registry, 2011–2018"
Our attention is grabbed by the first line of the report summary --
"This is the first ever paper from the National ALS Registry to report on the state-level prevalence of ALS within all 50 states of the US."
Wow. And there's a map. Our eyes are naturally drawn to the map to see how our states rank. Or to see how states where our loved ones with ALS have lived stack up.

But what they show us in this paper is not prevalence. It's just not. The CDC can slap a label on a table or a map that calls something "prevalence," but what they are showing us is not what is defined as the total number of individuals in a population who have a disease at a point in time. What they show us are the people with ALS whom they found. And they miss a lot of people with ALS.
I live in Indiana, so my eyes went to the map and it seemed to tell me that I'm living in a state relatively low in ALS cases compared with the neighboring states. Yay. That light color seems like a reason to be relieved. The darker blue Ohio, where Mom grew up and lived long before her ALS, is higher, and Michigan, where she once lived, too, looks like the worst when it comes to cases of ALS.
But the map is terribly misleading.
You have to read the small print in the report and pay attention.

The ALS Registry combs government payer files looking for cases of ALS. It also allows people with ALS to self-enroll in an online portal. That's how it finds cases of ALS, and it doesn't come close to finding everyone that way. In the 2017 data, a model estimated that it was only finding 44% of cases with these methods. In 2018 it did better but still missed an estimated 8159 people with ALS nationally, and they have no information about where those missing people live. Why would you publish a map of where all the people with ALS live without those missing 8159 people?
The numbers labeled as "prevalence" in this new state report only include the cases the registry found. They simply do not account for the estimated shortfall.
Any state that does a good job of recruiting self-enrollment in the CDC ALS Registry is going to look dark blue like Michigan. It's quite likely that my ALSA Indiana Chapter did a poor job of encouraging people to enroll in the CDC Registry. The color of a state has nothing to do with the actual prevalence of ALS in that state. It only reflects the cases the registry found in payer files and via self-enrollment. The missing cases are missing, and we have no idea how many cases are missing in each state.
And when you realize this, you see the comments about the northern trend of ALS prevalence to be just silly. And misleading.
It's not prevalence and calling it "prevalence" is wrong. And misleading.
This paper simply gives a reflection of found cases, but that's a far cry from all cases.
The paper could be informative as a tool to encourage self-enrollment in the lighter states, but instead, it presents a misleading narrative.
People who are interested in ALS and their environment should not have to scour the small print to realize what a map is really telling them.
This does not better describe the prevalence of ALS in the United States. It doesn't provide prevalence, period.
And the next time an ALS organization tells us to ask for a generous appropriation for this project, how about having a candid discussion with them about this misleading report first?

It's so important to families dealing with ALS. It's what keeps many of them going. You hope for a better day tomorrow. You hope for an effective treatment. You hope for a miracle. Hope is more precious to you than almost anything. You look for it everywhere.
Today, thousands of families dealing with ALS have found hope in an investigational therapy called NurOwn being developed by Brainstorm Cell Therapeutics, Inc. It is the beam of light they have sought every day they deal with the stinking ALS.
Brainstorm completed a Phase III trial over three years ago. If failed to meet its endpoints. It failed royally. Unfortunately many ALS trials do.
NurOwn represents a huge amount of hope because many of us have seen people who were in the trial actually feel improvement. That is literally miraculous in ALS. Unfortunately every time we go back and look at that summary report from the trial, the trial failed. But hope in ALS Land isn't easily smothered when something good has happened to someone. That hope is precious to thousands.
Through social media and a lot of hype, the hope has grown and reached thousands more people. And then thousands more.
But every time we go back to that report, the trial was a failure.
Brainstorm didn't step up and run another trial on those it suspects are the responders. Instead it decided to rearrange the data from the trial and convince us that they have the hope that every person with ALS seeks. If you remove the people that NurOwn didn't work for, it works! That's not great science, but it sure stokes the hope business.
And there have been all kinds of excuses for not doing another trial or providing expanded access to their unapproved therapy. People don't want to challenge those excuses. They don't want to mess with the holder of their hope.
For the last three months, since I made a comment quoted in a national publication that I suspected that the reason for never telling their trial participants (from a trial that ended in 2020 and has added no new data since) if they got placebo or treatment might have something to do with some of the public miracle cases having received placebo, my online life has become nothing short of a nightmare. Clearly many think I deserve it because I'm being critical of their ray of hope.
No, I'm being critical of a company that is holding their hope hostage.
I've learned a lot about adult cyber bullies. I've learned even more about parents and grandparents who teach the kids to be kind and then say some terrible things about another person online. They see me as stealing their hope -- a hope that they feel is so close to delivering them their miracle.
In reality, there is much that Brainstorm could have been doing to deliver some of the fruits of that hope sooner and to offer some scientific proof to back up the miracles. They have instead decided to hold hope hostage for one and only one ransom -- FDA approval to sell NurOwn to people with ALS at a price of their choosing.
Today, September 27, there is an FDA Advisory Committee meeting to help the FDA make its decision.
Two days ago we first saw the documents related to that meeting. The FDA briefing document was stunning. It took me hours to wade through the problems they found in Brainstorm's data, and perhaps of even more concern, the problems in their manufacturing processes. The normally noisy online ALS world supporting NurOwn was quiet. Journalists were busy pumping out coverage of a remarkable document. I suspected that the NurOwn supporters were reading and stunned, too. Silly me.
Yesterday we saw organizations completely ignoring the FDA briefing document and doubling-down on supporting approval. Didn't they even read what the FDA had found? Perhaps they don't want to be the ones to suggest we refuse to pay the ransom of approval of a product that represents precious hope but does not represent good science yet.
An online mob thinks I am trying to steal their hope. Brainstorm says the only way to get the hostage hope out of that room is FDA approval.
Today we will see people critical of anyone (including the FDA) who wont capitulate to the company that holds their hope hostage. The facts won't matter
I wish that more people would actually read the reports and think for themselves.
A company is holding their hope hostage rather than having used the last three years to find the scientific truth.
All with ALS deserve better than hope that isn't moored in truth.
Dear Advisory Committee Advisors, FDA Staff, and, yes, Brainstorm Cell Therapeutics Management,
As you know from hundreds of other comments, ALS is an awful disease. It's just awful. We lived the nightmare with Mom in 1997. It's not substantially better today. People with ALS deserve more options than the few they have.
They deserve access to investigational therapies. People with ALS should not have to wait years (literally lifetimes) for successful clinical trials and FDA approvals before they can try experimental treatments that have been proven safe.
Many have recently been convinced that the answer to access is to simply change the adjective from "investigational" therapy to "approved" therapy and let the company sell the therapy as if it had met the evidentiary standards for an approval. I respectfully disagree. Companies should provide access, and they have Expanded Access tools that the FDA provides until they establish efficacy.
We run Phase 3 trials for a reason. If we are not going to believe them, then let's not waste the tremendous amount of time and money and human commitment spent on them.
The NurOwn (debamestrocel) trial took three years, and it seems the company has then spent the next three years telling us not to pay attention to the trial. Six years. They could have run another Phase 3 trial in the last three years that might have focused on one of their suspected responder groups. Had they done so, we wouldn't be in the pickle that we are all in today.
If the FDA finds that the existing evidence supports approval, fine.
But if we're lowering the bar for Phase 3 evidence so far that we're completely ignoring the facts from that trial, then I think we're taking the idea of regulatory flexibility past its elastic limit. Springs that have been stretched too far don't just bounce right back.

We can't afford to make FDA approvals a charade when it comes to efficacy.
Access and evidence are both critical, and I appreciate that we have a regulatory system that can and should support both.
Thank you for listening.
The ALS clock is running.
In the next few weeks, the FDA will make a decision regarding approval of NurOwn for ALS.
Either way, another trial will be needed, so let's get moving.
If NurOwn is approved
Another trial will still be needed to confirm efficacy.
It is unlikely that payers will step up to pay for the therapy, so the confirmatory trial will be one path to affordable access (albeit with potential placebo exposure) for those who cannot self-pay. For those who can self-pay or raise funds or get insurance coverage, they will be able to purchase commercial access to the therapy.
If NurOwn is not approved
Another trial will be needed to produce efficacy data.
The trial will provide access (albeit with potential placebo exposure again) to those who can get in, and an Expanded Access Program (EAP) can provide broad access for those who cannot get into the trial.
"We can't afford it" need not be a Brainstorm excuse.
There are public funds available to help them via Act for ALS.
And Brainstorm can use the cost-recovery option allowed for EAP in order to remain whole while offering Expanded Access. People with ALS would still have to pay, but it would be cost only, without any profits that they would be responsible for with an approved product.

All roads lead to another clinical trial. Let's get going.
We can't afford another three years of rearranging existing data. We have seen anecdotal evidence of efficacy that makes it unconscionable to horse around any longer.
Let's get on with it and run the trial and provide access to people with ALS who want access. Now.
At the risk of giving some recent nonsense any more oxygen, I think it's important to document a few things.
I try to live by the "never wrestle with a pig because you both get dirty and the pig likes it" rule.

We have a Santa Claus problem.

We lost Sandy Morris to the stinking ALS this week.
As many of you know, she was a huge influence for the better in what we called ALS Land. If you didn't know her, just google "Sandy Morris ALS."
I've been working at ALS advocacy for a quarter century. I'm just one of many, and I work hard pounding away at the boulder. Sandy made the boulder crack.
Sandy made everyone involved in the fight against ALS better, from us simple advocates to top researchers and heads of state. People knew her and admired her and listened to her because she was right and did not cling to anything of the past as good enough.
Keep in mind that people come along in ALS Land and push the envelope all the time, but seldom do they make a significant dent in anything. I knew Sandy was the real deal on July 12, 2018. ALSA held a meeting in Washington to talk about the FDA ALS Guidance (again). Many of us were tired of talk, but a group of esteemed scientists and people living with ALS were assembled and talked some more. During a Q and A a woman from California called in and asked why we didn't just play the transcript from the February 25, 2013 hearing on ALS because we were just rehashing everything that had been said then. Boom. I knew that Sandy Morris from California was the real deal.
Many of us miss her terribly this week, mostly as a friend, but also as a leader. Sandy knew how to run a meeting. She had charisma, but she didn't depend on that. She always had an agenda. We always started on time and finished on time and every person understood the homework to be completed before the next weekly meeting. Sandy had vision and the human skills to manage projects to move to that vision. How we miss her.
The tangible accomplishments Sandy delivered are immense, and nobody paid her a dime to do what organizations and staffs have never been able to deliver. Expanded Access started to happen in ALS Land because of Sandy. She studied, always wanting to have her facts straight, then she acted with purpose. Legislative efforts were effective because of her relentless efforts. And drug developers started to design more humane trials because Sandy insisted and taught us all how to insist. And the Morris ALS Principles will set the tone and boundaries that have never been established before for those dealing with ALS.

Sandy was also a talent scout for ALS Land. She had people skills that brought some immense talent into the fight to work along side her.
We have a huge void in ALS Land this week. One person can't fill it. I just hope and pray that we can all chip in the talents we have to keep making cracks in that boulder that Sandy started so well for us.
We muddle ahead in a grief fog this week, but we have homework that is due next week. And we must deliver.
We sign forms. We agree to things in order to get treatments, both approved and experimental. It's exactly the same thing as signing forms in order to rent a car. There is a lot of fine print and there are things in that fine print that we don't particularly like (if we have the time and eyesight to read it), but what can you do? The form is a barrier between you and what you need. You sign to get past that barrier. You have no power in the deal when you are at the car rental counter.


The work goes on behind a big, heavy, black curtain.
Imagine a big corporation designing and delivering a new car. There are dozens of sub teams on the project and there may be contracted engineers and test drivers. Government regulators having a role to play, too. Do you think that any of those project members gets to go hide behind a big black curtain and do whatever they do, only to come out whenever they get finished? Do you think that the team is hidden from what others are doing? Do you think that somebody who needs more time just gets to take more time and tell others to wait?
Ha.
Even airlines figured out that a flight delay without a reason is disaster for their gate agents. Tell the waiting stakeholders what is going on.
In the often dysfunctional world of ALS, we have therapies being tested, analyzed, and evaluated for approval. Is anybody really back there today? We have no idea of what is going on. We just wait. And if nobody is actually back there doing something, we don't know if we're waiting for something that will never happen. We just wait.
I'm not asking for gigantic regulatory or process upheaval. Simply provide some basic transparency. What is going on behind that black curtain. Who are we waiting for and what are they doing. We realize that some jobs are difficult and take a long time. Just tell us what's going on. Are contracted statisticians working on data for the next three weeks? Are regulators analyzing public comments for three days? Are executives meeting with investors for a two-day conference? Are we waiting for an investigator's hernia surgery? What is going on? Or what is not going on?
The mystery of the black curtain gives an awful lot of cover and leads to a lot of misunderstandings.
Just open the $%^&* curtain and tell us what's going on.
Below are my comments submitted to the FDA Advisory Committee that will be meeting to address questions related to the Amylyx AMX0035 approval.
_____
Mom was diagnosed with bulbar-onset ALS 25 years ago at age 78 (after a long delay to diagnosis). She had a fast case and died in 1997.
One might think that a therapy option that slows the speed of a difficult terminal disease might not be of much use to an elderly person in her situation. I think that just the opposite is true.
One morning, for the first time ever, she asked me to help her button her blouse. She had strength in her hands but was losing finger dexterity. As I buttoned those few buttons, she said, "Do you know what the worst part is?" I simply said that I did not. She then said, "Once I lose the ability to do something, I know I'll never be able to do it again."

She had buttoned her last button.
I think we all need to let that soak in.
She took riluzole without any pretense that she was going to beat the grim reaper. She simply wanted to try to keep the independence and dignity of being able to button a button or take care of her personal hygiene as long as possible.
My understanding is that AMX0035 hit its primary endpoint with statistical significance and has a good safety profile. It's a combination of substances that the FDA knows well. We are realistic that not every therapy will work for every person with this wicked, heterogeneous disease. I think AMX0035 belongs in a physician's toolbox to try to help a person with ALS who isn't ready to throw in the towel on buttoning that last button.
Thank you very much for the opportunity to comment at an important regulatory moment. This is the time to apply both the spirit and the letter of the FDA ALS Guidance.
You can lead or you can choose to continue to mislead. The choice is yours.
ALS Prevalence and Incidence in the US
Option 1: Mislead.
This is unfortunately the path you have chosen.
We sporadically get prevalence reports based on the people with ALS you find rather than the population of people with ALS in the US. You do not have a population-based registry, yet you issue reports with demographics as if you do.
There are some important examples of how misleading you have been in the past few months --
Dr. Walter Koroshetz, the head of NINDS at NIH, testified the following to Congress in July, 2021:
https://docs.house.gov/meetings/IF/IF14/20210729/113983/HHRG-117-IF14-Wstate-KoroshetzW-20210729.pdf
"Neurodegenerative disorders also include rare but devastating conditions like ALS, a rapidly progressive, fatal disease that affects the nerve cells controlling voluntary movement. The CDC estimates that 12,000–15,000 Americans have ALS, and approximately 5,000 Americans are newly diagnosed with ALS each year."
You misled one of the top neurologists in the country, and as a result you misled the Congress.
News outlets also turn to the CDC as a trusted source.
https://www.wdtv.com/2021/07/28/morgantown-resident-talks-about-living-with-als/
"Amyotrophic Lateral Sclerosis (ALS) affects between 12,000 to 15,000 people across the U.S., according to the CDC."
https://khn.org/news/article/dying-patients-with-rare-diseases-struggle-to-get-experimental-therapies/
"More than 16,000 people in the United States were estimated in 2015 to have ALS..."
More than 16,000, indeed. Way more.
And there is the draft scoping document that ICER produced for their study on pricing related to two anticipated FDA product approvals. ICER is in the numbers business and turned to the CDC for a very basic number.
https://icer.org/wp-content/uploads/2022/02/ICER_ALS_Draft-Scope_020222.pdf
"There are about 16,500 people living with ALS in the United States, with a prevalence of 5 to 6 per 100,000 persons."
ALSA issued comments related to this draft but failed to mention the understatement of prevalence of ALS by the CDC. ALSA is a "partner" (another misleading word since ALSA is actually a paid contractor on the project) and for some reason decided to be misleading, too, by ignoring the problem. Thank heavens ICER did correct the data based on an individual pointing out the incompleteness. of the CDC's data.
Option 2: Lead
Stop publishing prevalence (and now incidence) reports as if your data are complete. Be clear that this is a sample of the people you found and you don't know what you don't know. The people you didn't find don't necessarily look like the people you found. And based on a past analysis, you miss almost as many people with ALS as you find. Be clear. Give us details that are actually meaningful such as how many people self-enroll, how many are in the Medicare files, etc. And please publish data. simply and promptly. Leaders understand the importance of meeting due dates.
Clinical Trial Notification
Option 1: Mislead
Again, this is the path you have chosen.
People are encouraged to sign up for clinical trial notification and they infer that you will let them know of trials. They do not understand that you will inform them of a tiny fraction of enrolling interventional trials. They sit back, relax, and wait for the magic email from the CDC telling them of the right trial while their eligibility windows evaporate.
And your matching capabilities are limited. The fact that dead people can receive trial notifications is a testament to that problem.
Option 2: Lead
Stop using 1980 email tactics. You have access to a list of all enrolling interventional trials via clinicaltrials.gov. Work with your "partners" to design trial notification that is more effective and less onerous than yours. The best way may not involve you at all. That's fine. We need what is best for those with ALS and sponsors.
Summary
In an attempt to constantly celebrate success of the project, it has been easy for you to mislead. Please stop.
The CDC and ATSDR should lead, and that means being honest and. clear about what we have and what we need to do.
Please lead.
During the past week I have worked on finding the status of multiple ALS research projects. You know, the ones that were hot topics ten or five or even just three years ago. What ever happened to them? What is going on with them today?
I find the grant information. Then I find scant published results.
The most troubling part is that it feels like projects morph from their original designs into something very different. Maybe that drift is fine. Maybe it's like converting an old shoe factory into a factory making cell phone cases. But how do we know what is really going on in there?

It feels akin to an industrial complex that was built helter-skelter. New buildings are built to manufacture new things, but rather than having a cohesive architecture, we have dozens of individual plants with their own styles. We have leaders who know how to do their work best in their own buildings.
Modern factories use colocation to leverage efforts among small manufacturers to minimize duplication of efforts ALS researchers work in their own expensive silos. And their promises of collaboration involve moving data back and forth, much like old factories used to move materials through arcane chutes and rail cars.
What is wrong with this picture?
So much is wrong.
And it is paid for by generous donors and taxpayers. The litter of past research projects is as real as the litter of old factory buildings, and it is every bit as expensive.


- A Natural History Study
- A Broad Network of Clinical Trials
- A Framework for Broader Insights - A Parallel Track
- NIH Leadership
- Our Relationship



I write you as a concerned advocate for those with ALS (we lost Mom to ALS in 1997), a person who believes in the value of epidemiological data in science, and a taxpayer.
ATSDR has administered a CDC ALS Registry since we worked hard to have the ALS Registry Act passed into law in 2008. It has disappointed in many respects -- undercounting cases yet publishing reports as if counts were complete, terribly late reporting of data (we just saw 2016 data for the first time), falling into the distracting temptations of scope creep, and entangling itself in financial relationships that prevent objective and candid oversight.
You wisely inserted language into the recent appropriations bill --
https://docs.house.gov/
Amyotrophic Lateral Sclerosis Registry.—The Committee directs CDC to present a plan to the Committee within 90 days of enactment of this Act to enhance the oversight and advisory process for the National ALS Registry to increase transparency and better reflect the needs of the ALS community. This plan should consider ways to translate Registry findings to human application that can lower the risks and disease burden of ALS, make disease reporting more representative, more accurate, and more inclusive, and include a range of estimates rather than point estimates of ALS prevalence. Equally important are updates to the survey process to ensure the data they collect are impactful and respectful of participant burden. Finally, the plan should ensure that the ALS community can view as much Registry information as possible without compromising the privacy of participants.
Two weeks ago the CDC ATSDR Registry folks held an annual meeting. It has never been a true oversight meeting. Two weeks ago it was more of a closed, clubby celebration of questionable achievements (from what little I was able to see). The public could only watch part of the first day. It takes an invitation to be a full, two-day participant with the ability to unmute and ask questions and make comments. We're not sure what it takes to get an invitation. A man with ALS, Stephen Finger, PhD, who has participated for several years and asks good questions was not invited back this year. He seems to have outlived his welcome. Good for him, but his exclusion was revealing.
ATSDR refers to its many "partners" at the meeting. Those are largely paid contractors, including the ALS Association (ALSA), the Muscular Dystrophy Association, and Les Turner ALS Foundation who together get around $1,000,000 per year in no-bid contracts for some vague "education and outreach." ALSA is also the lead advocacy organization that lobbies you for the $10,000,000 annual budget for the project.
Add to that a number of grant recipients and potential grant recipients at the meeting, and we have a pretty good recipe for a love-fest rather than any kind of objective oversight.
Please insist that they bring to you an oversight plan that is composed of third parties with knowledge of epidemiology and payer data and information systems who have no financial ties to this project.
Thank you very much.

We've had a lot of anticipation and waiting since we worked hard to have the ALS Registry Act passed in 2008. Has it been worth the wait?
We're close to the annual CDC ALS Registry meeting on August 31 and September 1, 2021. It's not an oversight meeting. The description is more of a celebration -- "Update stakeholders on the progress and achievements of the National ALS Registry." Please register and tune in if you are able. You've paid well over $100 million for this Registry. Has the ketchup been worth the substantial waits?
The primary purpose of the Registry as written into the law is "to better describe the incidence and prevalence of ALS in the United States." Everything else is mustard or relish.
Back in the 20th Century we were promised a passive data mining technique that would find 85% of ALS cases via this data mining, and then the other 15% could be added by a patient self-enrollment portal. We would get annual reports after a time lag necessitated by the wait for public payer files. That was the promise.
The waiting and the ketchup have been particularly troublesome in the last three years.
The Waits
We have not received any semblance of annual reporting. The cavalier attitude about due dates really puts the value of the output into question. The 2016 data were just published this week.

Heinz knew when to completely redesign that ketchup bottle. We now use 21st Century bottles that eliminate the wait. Perhaps it's time for a significant 21st Century bottle change for the Registry.
The Ketchup
The hit-and-miss prevalence reports have questionable value. The undercount is significant. The demographics continue to be published. It is not clear that these are merely the people that the Registry finds, and there may be just as many people with ALS out there whom they missed. Two top NIH officials at a recent Congressional said that according to the CDC there are 16,583 people with ALS in the United States. We repeatedly see the CDC number as being the number. First do no harm. These prevalence reports are doing harm by misleading the public about the number of people living with ALS.
A recent study by Miller et al used some different data sources to estimate prevalence that was starkly different from the CDC's. And the authors were able to be much more timely than the CDC.
If the ketchup coming out of the bottle isn't what the consumer expects, Heinz knows to change the recipe.
The Recipe
The "FAQ" document that came with this week's publication of the 2016 prevalence report causes major concerns about the recipe.
They are cooking in excuses for even more delays. That's not acceptable, especially with the trail of inconsistent excuses we've had in the past.
They are cooking in excuses for a flawed design. They knew full well that ALS was not reportable or notifiable back when they made promises and designed the algorithm for passive data mining and the patient portal.
They suggest buying data from more sources and adding them to the recipe. Whoa! It's time to step back and do some test recipes first. Figure out what gaps new data sources can or cannot fill. Design before you start buying ingredients. We've been asking for years for their "partner"/contractors to supply counts on the numbers of unique people with ALS they served in the past year along with counts of how many of those were new. Every year this has been completely ignored. Finally, the CDC seems curious. Look at the numbers first, please, before you enter into more entangling contractual relationships that may not actually be the best solution for the completeness problem! They've never been in a rush before. Why rush into implementation without a smart analysis? Perhaps there are even some prepared products that could replace some of the old infrastructure.
They also are suggesting that the capture/recapture approach will be the magic spice to make the ketchup better. That's not necessarily true. A 2013 report challenges the magic for this project if you read it carefully.
The Other Condiments
The ketchup hasn't been good and certainly hasn't been worth the waits.
When insights into incidence and prevalence are questioned, the project fathers often change the focus to all of the other things that a generously funded government project has done. The mustard and relish become more important when the ketchup isn't good. How do they measure success of every add-on? Number of emails sent does not make a great trial notification system. Number of biospecimens collected does not make a great Biorepository unless we have tissue and data representative of the diverse population of people with ALS.
It's quite possible that the external research grants are the most valuable contribution that this project makes; however, the grant making process is opaque to the public and we can't even find out how much of the $10,000,000 that this project costs taxpayers is used by these grants.
Nobody at the annual meetings seems curious about the expenditure in general, let alone on functions like trial notification or on the Biorepository or the CME or the prevalence reporting.
The Ketchup Consumer
Some consumers have questions that never seem be asked at the annual meeting. We pay $10,000,000 per year even if the ketchup isn't delivered and we pay regardless of the quality that finally comes out of the bottle. We should be asking questions.
1. How many unique people with ALSA, MDA, LTALS serve last year? How many of those were new cases?
2. CDC has given ALS, MDA, LTALS annual contracts that total around $1,000,000 (10% of the annual appropriation) for "education and outreach." How does the CDC come up with those contract amounts? How does CDC measure those contractors and deliverables? What is the cost/benefit evaluation?
3. Does ATSDR have any idea how much the Biorepository costs every year? The trial notification? The grants? How do they measure the cost versus benefit?
4. Is ATSDR not concerned about the incomplete prevalence count that has been taken out of context in public media? People, even top NIH professionals, have quoted the 16K number as the number of people in the US with ALS. Is this not a concern?
5. The Miller paper underwritten by MT Pharma found half of its people with ALS in private payer files. That's pretty much the smoking gun that the surveillance of public payer files will not be successful. How did that paper's authors get data in a much more timely manner than ATSDR? They reported data through 2017 in June of this year.
6. Earlier this year ATSDR received a suggestion to just publish tables of data in a regular annual process so that the report and publication process aren't delaying things. Again, how about simplifying the process and just providing data tables in a regular and more timely manner?
7. How many people are represented by the Biorepository? How many of them are living? What are the demographics of people represented?
8. How often are Registry data matched with the death index data? There are reports that deceased people continue to get clinical trial notifications. That is painful and does not speak well to the matching capabilities of this rudimentary emailer.
9. A 2017 report raised concerns about disparities, equity, and inclusion in Registry data. What tangible actions have been taken to address and measure these?
10. ALS has a cruel way of imposing term limits on the invited people with ALS who are allowed to speak at your annual meeting. We have lost Ted Harada, Rob Tison, and Becky Kidd among others, all experienced people who thoughtfully prepared and spoke their minds at your meeting before they died from ALS. Your decision to change the rules in 2021 so that Stephen Finger could no longer participate smacks of wanting to eliminate a thoughtful, prepared person with ALS who spoke his mind and perhaps outlived his welcome. This is not a question.